Busulfan: A Deep Dive into Its Legacy, Function, and Future
Historical Development
In the early 1950s, researchers searching for treatments for chronic myeloid leukemia (CML) stumbled upon busulfan, a discovery that changed the landscape for both patients and hematologists. Early experiments revealed busulfan’s power to target bone marrow cells, shrinking tumors and suppressing the overproduction of abnormal blood cells. By the middle of the century, this compound became a mainstay for CML treatment. Over decades, newer therapies have come along, but many clinicians still respect the history busulfan brings—its ability to wipe out bone marrow remains crucial, especially before stem cell transplants.
Product Overview
Busulfan, often sold under names like Myleran and Busulfex, serves mainly as an alkylating chemotherapeutic agent. Its main role involves conditioning patients before bone marrow or stem cell transplants, attacking both malignant and healthy bone marrow cells to clear the way for donor tissue. You’ll find busulfan in both oral and intravenous forms, each prepared under strict guidelines to handle its potency and ensure safe patient outcomes. The drug stands out not just for what it does but for the concentration required for effect and the delicate balance health care teams must strike between destroying disease and managing risk.
Physical & Chemical Properties
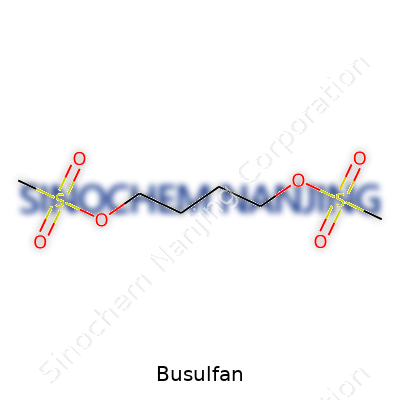
Busulfan appears as a fine, white crystalline powder, odorless, with a slight bitter taste. Solubility plays a practical role in clinical settings: the drug dissolves slowly in water, more readily in organic solvents such as acetone and ethanol. The compound’s molecular formula, C6H14O6S2, points to two sulfonate groups, each capable of attacking DNA, crosslinking strands and halting cell division. Busulfan decomposes under heat and light, so storage in cool, dark environments remains the gold standard for stability. Its melting point hovers around 103 to 105°C, further demonstrating its stability as a solid under most ambient conditions.
Technical Specifications & Labeling
The drug comes with clear dosing instructions and lot-specific information on every vial or tablet blister pack. Most products list concentration in milligrams per milliliter for the solution and in neatly scored tablets for flexibility in oral dosing. Labels carry bold cautions: cytotoxic, handle with care, for hospital and specialist use only. Beyond that, technical data sheets include storage conditions, shelf life, and the presence of excipients or stabilizers in the formulated solution. Healthcare providers rely on these details not just for dosing accuracy but to avoid accidental exposure, a point that cannot be overstated with agents like busulfan.
Preparation Method
Manufacturers synthesize busulfan by linking 1,4-butanesulfonic acid chloride with the corresponding alcohol, followed by purification through crystallization and careful drying processes. Rigorous quality checks ensure the absence of impurities that could alter its pharmacokinetics or lead to hazardous byproducts when injected or ingested. Scale-up from lab to industrial preparation demanded specialized containment and ventilation, as the vapor of intermediate chemicals exposes workers to respiratory and skin risks. Each production lot undergoes analysis for purity, potency, and stability before release, reflecting decades of refinement and regulatory scrutiny.
Chemical Reactions & Modifications
Busulfan’s hallmark sits in its alkylating action: each methanesulfonate group seeks out guanine bases on DNA, forming stable crosslinks that halt the cell cycle. As research expanded, chemists modified the structure to tune its reactivity, seeking analogues with potentially better selectivity or altered metabolic profiles. Many experiments aimed to bolster water solubility while keeping cytotoxic power, hoping for less toxicity outside target cells. The original molecule’s reactivity also raises flags for safe handling: improper mixing with other drugs or excipients creates risks for decomposition and loss of potency.
Synonyms & Product Names
Around the world, busulfan goes by several names, each linked with local regulations or branded formulations. Myleran, its most recognized trade name, marked early use in oral form. Busulfex emerged later for intravenous protocols, claiming more predictable absorption. Other identifiers crop up in research or procurement channels—“1,4-butanediol dimethanesulfonate” serves in chemical registries, while “BSF” often appears in shorthand among clinicians. Each synonym connects to the same molecule, but patients, regulators, and pharmacists quickly learn the importance of distinguishing between formulations and dosing forms.
Safety & Operational Standards
Handling busulfan calls for specialized training, as exposure risks run high for healthcare workers. Personal protective equipment—gowns, gloves, goggles—becomes mandatory during preparation. Pharmacies mix the injectable form inside biological safety cabinets, with air filtration that can trap volatile residues. Most institutions mandate double-checks before administration, ensuring correct patient, route, and dose. Waste handling, too, falls under close watch, usually via sealed bags for incineration. Regulatory agencies classify busulfan as hazardous, mandating clear record-keeping and periodic audits to check compliance with safety protocols.
Application Area
Busulfan’s strongest role shows up in the preconditioning space for bone marrow and stem cell transplants, especially for patients fighting leukemias and lymphomas. Hematologists have leaned on busulfan for decades, using it to wipe out diseased marrow and suppress the immune system long enough for donor grafts to take root. Some studies explore its role in other cancers or as a bridge for autoimmune conditions. Experience at the bedside proves that while targeted cancer therapies have grown, busulfan offers a proven route for high-risk or relapsed cases, particularly when disease crowds out hope for less aggressive options.
Research and Development
Busulfan’s journey through research labs reads like a roadmap of cancer drug evolution. Early trials looked at dosing schedules for maximum cell kill and minimum side effects. Later years saw geneticists explore how individual enzymes metabolize busulfan, guiding pharmacogenomic dosing strategies that tailor regimens to patients’ DNA. Ongoing projects include trials pairing busulfan with immunotherapies, investigating whether a wiped-out marrow boosts the effect of donor-derived immune cells. Some researchers push for new delivery vehicles—liposomal carriers or nanoparticle suspensions—seeking ways to target the drug and spare the gut or liver from collateral damage.
Toxicity Research
Busulfan brings heavy baggage: liver veno-occlusive disease remains a serious complication, sometimes fatal, as does severe suppression of blood counts. Lung fibrosis, seizures, and secondary cancers have all turned up as long-term risks, especially at higher doses. Animal studies point to a narrow therapeutic window; even in tightly monitored clinics, overdoses or rapid infusions have led to organ failure. Monitoring blood levels—therapeutic drug monitoring—has now become standard at many transplant centers, allowing tweaks in real time to balance disease eradication with side-effect management. Without dedicated teams and careful attention, toxicity outpaces benefit in a flash.
Future Prospects
The future of busulfan stretches into several promising directions. Personalized medicine spurs efforts to link busulfan dosing with rapid genetic testing, fine-tuning exposure to individual enzyme activity and minimizing organ damage. Next-generation analogues and prodrugs in development hope to overcome problems with current formulations—perhaps with better solubility, more predictable kinetics, or safer breakdown in the body. As cancer therapy crowds with targeted options, busulfan may find its niche in combination regimens that take advantage of its marrow-clearing potency without facing off alone against diseases that adapt and mutate. There’s experience behind every dose, and innovation picking up where tradition meets challenge.
What is Busulfan used for?
Understanding Busulfan and Its Role in Cancer Treatment
Busulfan shows up in hospitals as a chemotherapy drug. Most people crossing paths with it are either dealing with certain blood cancers or supporting someone who is. This medicine’s main job is to wipe out fast-growing cells—usually those causing trouble in conditions like chronic myelogenous leukemia (CML). Some folks hear about it before a bone marrow or stem cell transplant, where Busulfan works to clear the body’s old bone marrow.
My Experience Seeing Its Impact in Cancer Care
I’ve heard several stories from family members and friends tangled in the world of blood cancers. Watching someone face this kind of treatment never feels easy. Busulfan often enters the picture right before a transplant. Its role is to knock down the body’s immune cells so new, healthy cells have a fighting chance. For many battling CML, blasting away stubborn bone marrow is a crucial first step if they want a shot at long-term recovery.
Cancer doesn’t care about plans or timing. Many folks hit by it get stuck with drugs that don’t pull any punches, and Busulfan is among those heavy hitters. Doctors favor drugs like Busulfan for one clear reason: they knock out the disease when other options aren’t working well enough.
Busulfan Isn’t Just for Leukemia
This drug doesn’t stick to one lane. Doctors sometimes reach for it to treat other blood disorders, like myelodysplastic syndromes or even some sickle cell cases. For each of these conditions, Busulfan’s purpose stays pretty much the same—destroy diseased bone marrow and help introduce new, healthy cells. Occasionally, it pops up for some rare childhood disorders as well.
Facts Behind Its Use
Busulfan has been around since the 1950s. Over the years, it stuck as part of many conditioning regimens before transplants. The National Cancer Institute recognizes it as a standard option. Several big cancer centers give out Busulfan as part of “preparative” or “conditioning” therapy. Survival rates for certain leukemia patients have gone up since doctors started pairing Busulfan with other drugs like cyclophosphamide.
Still, this drug does come with baggage. It can knock out infection-fighting white blood cells, leading to risk of severe infections. Other troubles, like liver problems or lung scarring, have made headlines over the years. This medicine isn’t passed out lightly—patients usually get hooked up to lots of monitors, and every dose gets calculated down to the last decimal to limit bad reactions.
Moving Toward Safer, Smarter Treatments
Patients and doctors crave safer options. Some new regimens use reduced doses or different combinations to cut down on risks. Research teams at institutions like MD Anderson and Memorial Sloan Kettering continue to test better ways to limit side effects, like swapping out Busulfan for newer drugs in some situations or using targeted dosing based on a person’s size and metabolism.
Having personally watched people go through transplant prep, I understand the desperate need for less harsh treatments. Clinical trials push forward every year, and more precise, tailored dosing tools are slowly making these treatments less brutal. Still, for many today, Busulfan stands as a bridge to another chance. Knowing what to expect—and which questions to ask—remains just as important as our hope for newer, kinder therapies in the future.
What are the common side effects of Busulfan?
What Patients Face While Using Busulfan
My time supporting cancer patients and connecting with families enduring treatment has shown that Busulfan comes with a heavy set of side effects. Used mostly in bone marrow transplants, this powerful drug often leaves visible marks on people’s bodies and spirits. Chemotherapy fights hard, and so do the people receiving it. Commonly, Busulfan packs a punch on the blood. After a few days or weeks, many see their white blood cell counts fall. This leaves folks wide open to infections. Some catch fevers, or simple colds turn dangerous fast. People might not always spot the warning signs, so frequent checkups help catch problems before they snowball.
Besides hitting white blood cells, Busulfan can cause a strong drop in red blood cells and platelets. Fatigue creeps in, as if every step needs more effort. Bruises and nosebleeds can appear out of nowhere. My conversations with nurses show they stay on watch, checking skin for odd spots and carefully measuring even small bleeding. In hospitals, teams keep close tabs on blood values and give transfusions when numbers tumble.
Unpredictable Nausea, Mouth Sores, and Hair Loss
Stomach trouble comes up frequently. A lot of people get hit by nausea, even with the best anti-nausea meds. Some mention food tastes bland, and times at the table can become a struggle. In my own experience helping friends with chemo, bland rice and crackers became daily staples. Drinking enough water and sipping ginger tea sometimes eases the worst of the waves.
Sores along the gums and mouth add to the discomfort. For many, these ulcers make speaking and eating a challenge. Doctors usually recommend gentle mouth rinses and careful oral hygiene to help with this. Losing hair, either all at once or in clumps, makes the road tough for some. Hair often grows back, but the shock and sadness never feel simple or predictable. Support groups and honest talks about appearance changes help ease these worries for people coming to grips with treatment.
Impact on Organs and Hidden Risks
Beyond what you see on the outside, Busulfan can work its way into the liver and lungs. In rare but serious cases, people develop veno-occlusive disease, a type of liver problem. I recall hearing about folks swelling up, or skin taking on a yellowish color. The medical team moves quickly at the earliest signs. Keeping an eye on liver tests handles much of the risk, as does giving the lowest possible dose for the shortest possible time.
Lung issues pop up less frequently, but they shouldn't be ignored. Breathing troubles sometimes reveal deeper problems. People who already have lung troubles or autoimmune conditions need extra careful monitoring. Prompt attention to coughs and shortness of breath matter here.
Protecting People on Treatment
With any drug like Busulfan, the care team forms a safety net. Honest conversations carry a lot of weight. Many families keep a notebook handy, writing down new symptoms, so nothing slips through the cracks. Frequent blood tests and organ monitoring stand as common-sense steps. Small comforts like soft blankets, gentle foods, or a friend during appointments help more than most realize. Recognizing that Busulfan’s side effects often travel as a team—not just one at a time—makes it easier to prepare, respond early, and keep on living through it. Each challenge deserves attention, respect, and teamwork to get through the roughest patches.
How is Busulfan administered?
What Folks on the Cancer Ward Know
Stepping into a cancer clinic, most folks spot a nurse prepping an IV line and know something serious is happening. That’s the scene in most places where busulfan gets handed out. Doctors use this gritty medicine mostly for folks gearing up for a bone marrow or stem cell transplant. Nobody picks it for fun—busulfan’s for those who need help real bad. Once upon a time, there were chewable tablets, but now, IV infusions stand as the main road in, and there's a good reason for it.
Why the Intravenous Route Matters
Hospitals lean on the IV route because it's more precise than chasing a pill with a glass of water. The old pill forms could throw everyone's plans out of whack, especially for kids, folks throwing up, or anyone with swallowing trouble. IV eliminates all that, taking the gut out of the equation so the medicine hits the bloodstream in a predictable way. Doctors can measure the dose closely, then check if any side effects like low blood counts or changes in the liver crop up.
Tough Stuff: Dosage and Side Effects
There’s no one-size-fits-all rule for busulfan. Each person brings their own body chemistry, size, and previous treatment baggage. Oncologists spend a lot of time running bloodwork before, during, and after infusions to make sure the drug hits the right targets but doesn’t wreck everything else in its path.
Talking to folks in cancer centers, it’s clear that the mood changes around this drug. Some fear mouth sores and fevers; others have lost their hair or felt wiped out for weeks. The risks that come with busulfan—like damage to the lungs or liver—aren’t just scenarios you read in a textbook. Parents, grandparents, and kids all keep an eye out for these changes. Nurses hold your hand and say, “Let us know if something feels off,” because with busulfan, you can’t just shrug and wait.
Support, Information, and Teamwork Matter
Nobody can handle a cancer diagnosis and chemo alone. More than ever, people rely on strong nursing teams for support and solid information. Hospitals need to offer updates written in plain language so families know what’s going on. Clear explanations about busulfan—why it’s dripped in slow, why blood tests matter—make all the difference. Cancer treatment is a grind, and the only way through is with a team that steps up for each patient, every day.
What’s Next and Possible Solutions
Problems like long hospital stays, drug costs, and side effects bog down families. Clinical researchers push hard to develop safer ways to deliver busulfan and to help people recover faster after transplants. Some centers test out smaller, more frequent doses or look at how genetics change the way each body reacts. Others run support groups that bring together folks who’ve walked the same road. Even small touches—good communication, quick pain control, friendly faces—can help folks feel less like nameless patients and more like the strong people they really are.
One lesson sticks out: sticking to the science, being honest about the rough days, and drawing on support from loved ones and medical teams gets people through. Busulfan might be tough, but the team treating it with respect and clear information always gives patients the fighting chance they need.
Are there any special precautions while taking Busulfan?
Understanding What Busulfan Does
Busulfan serves a real purpose in cancer treatment, especially for those confronting certain types of leukemia or preparing for bone marrow transplants. This isn’t your everyday medicine. It works by slowing or stopping the growth of cancer cells, reversing the direction of the disease. Just like any powerful tool, it brings along some heavy duties for anyone taking it—patients, caregivers, and medical teams alike.
Watching Out for Serious Side Effects
Having spent time caring for a family member during chemo, I’ve noticed that drugs like busulfan demand careful watching. Side effects aren’t just a possibility—they’re part of the experience for many. Low blood counts, mouth sores, and fevers show that the body’s defenses can drop low. Studies from leading cancer centers report that busulfan’s biggest risks come from bone marrow suppression, leading to infections, unexplained bruising, and extreme fatigue.
Doctors take blood samples often for a reason. They want to catch infections early and watch how the medicine shifts blood counts. Once, my aunt’s white blood cells plummeted and she ended up in the hospital with a fever that wouldn’t break. Folks shouldn’t expect to just tough it out—any new fever or sign of infection deserves immediate medical attention. Hospitals often prescribe antibiotics up front, since a small cold can escalate quickly during treatment.
Avoiding Interactions and Toxic Reactions
Mixing busulfan with other medications isn’t simple. Many drugs, even over-the-counter painkillers or herbal supplements, can change how busulfan works. According to the Mayo Clinic, acetaminophen should get avoided for at least seventy-two hours before busulfan starts—this can help prevent unexpected liver stress. I remember one pharmacist spending nearly twenty minutes cross-checking every supplement my friend took before starting therapy, knowing that something seemingly harmless can spark a real crisis when cancer drugs are in play.
Pregnancy, Fertility, and Long-Term Planning
Busulfan isn’t just hard on cancer cells. It threatens fertility and can harm a developing fetus. Anyone trying to conceive, or their partners, needs to talk with a doctor about options—egg or sperm storage could be a wise choice before treatment. Birth control matters for both men and women while using busulfan and for up to six months after finishing. Researchers at the American Society of Clinical Oncology stress this point because accidental pregnancies during chemotherapy almost always lead to heartache.
Daily Choices Matter
Safe handling of busulfan protects everyone in the home. Family members often don gloves when dealing with spilled tablets or supporting someone after an infusion. Washing hands after handling, wiping down surfaces, and keeping the medication out of reach of kids and pets turns out to be less of a hassle than dealing with an emergency. On top of this, eating well, resting, and staying hydrated keep the body strong enough to handle the drug’s demands. My neighbor drank a lot of fluids and kept a simple, bland-food diet. It didn’t erase all discomfort, but it made each day a bit smoother.
Building a Support System
No one has to walk this road alone. Social workers, pharmacists, doctors, and family can share the load. Open conversations about side effects and emotions can shorten a long journey. Leaning on the experience of those who have walked the same path can ease both the body and the mind. Patients who prepare together with their care team—focusing on communication and safety—stand the best chance at getting through treatment with less fear and fewer setbacks.
Can Busulfan interact with other medications?
Everyday Risks with Powerful Medicines
Talking about chemotherapy always leads to tough questions. Busulfan treats some blood cancers by wiping out bone marrow cells so new, healthy cells can take root. Powerful isn’t always straightforward, though, and people using busulfan face a specific challenge: it can interact with other medications in ways that change how well it works or how safe it feels.
How Mixing Medicines Gets Complicated
Many adults living with cancer already take a handful of daily tablets for blood pressure, cholesterol, or pain. Busulfan moves through the body thanks to liver enzymes that, in reality, metabolize hundreds of drugs. So, something as common as acetaminophen or ibuprofen sometimes puts extra stress on the liver or changes how busulfan is processed. In hospitals, doctors look out for clear signs of trouble, but in the real world, these problems often sneak up.
I’ve seen friends and family members bring long lists of medicines to every doctor’s appointment. Every addition feels like playing a risky game because even drugs used to prevent infection, like antibiotics or antifungals, can shift the way chemotherapy unfolds. For instance, fluconazole and metronidazole both slow how busulfan leaves the system, increasing side effects like seizures. On the other hand, drugs like phenytoin, used to prevent those same seizures, actually clear busulfan faster, sometimes too fast for cancer treatment to work as planned.
Why Doctors Care About Details
Small changes add up. Chemotherapy does not just treat disease; it also puts stress on every other system in the body. So, each medication’s effect counts. Health teams scan entire medication lists at admission, but the pressure falls on patients to keep track of everything—over-the-counter pain pills, herbal supplements, even vitamins. I remember an oncology nurse telling me, “The only way I can help is if I know what’s coming in.”
People might think about prescription medicines first, but antacids, anti-nausea medicines, or drugs for anxiety can also get tangled in the chemistry. Someone taking busulfan who then starts an anti-fungal prescribed by another doctor could end up with liver strain or worse. During busulfan treatment, adding or removing a single medicine nearly always means discussing it again with a pharmacist or oncologist.
The Role of Clear Communication and Care Coordination
Avoiding dangerous interactions doesn’t just happen in the hospital. At home, patients sometimes bounce between primary care, specialists, and urgent care visits. Everyone writes prescriptions using different electronic records. Keeping a paper list or an updated phone note of every medicine—prescribed, purchased over the counter, or taken as a supplement—goes a long way. Bringing that list to every appointment might feel tedious, but it remains essential for catching dangerous overlaps.
Modern medicine relies on teams. Pharmacists run checks for known conflicts before people leave the pharmacy, but those checks only work if the whole story is available. Open, honest conversations—the kind where people say “Yes, I also started taking St. John’s wort for my mood,” or “I use Tylenol PM every night”—change outcomes. Each detail lowers risk. And every lowered risk means one less hurdle for people already fighting tough battles.
| Names | |
| Preferred IUPAC name | Butane-1,4-diyl dimethanesulfonate |
| Other names |
Myleran Myleran Oral Busulfex |
| Pronunciation | /ˈbjuːsəlˌfæn/ |
| Identifiers | |
| CAS Number | 55-98-1 |
| 3D model (JSmol) | `3D model (JSmol)` string for **Busulfan**: ``` MPD(ClCCS(=O)(=O)OCCCl) ``` |
| Beilstein Reference | 1710862 |
| ChEBI | CHEBI:3182 |
| ChEMBL | CHEMBL547 |
| ChemSpider | 5462 |
| DrugBank | DB01008 |
| ECHA InfoCard | 100.016.382 |
| EC Number | 211-669-2 |
| Gmelin Reference | 30104 |
| KEGG | D00210 |
| MeSH | D001322 |
| PubChem CID | 2477 |
| RTECS number | EO1360000 |
| UNII | 139D7V2S5B |
| UN number | UN2811 |
| CompTox Dashboard (EPA) | DTXSID9020670 |
| Properties | |
| Chemical formula | C6H14O6S2 |
| Molar mass | 246.306 g/mol |
| Appearance | White crystalline powder |
| Odor | Odorless |
| Density | 2.002 g/cm³ |
| Solubility in water | Slightly soluble |
| log P | -0.34 |
| Vapor pressure | 7.97E-8 mmHg |
| Acidity (pKa) | -0.4 |
| Basicity (pKb) | 3.87 |
| Magnetic susceptibility (χ) | -8.7e-6 cm³/mol |
| Refractive index (nD) | 1.489 |
| Dipole moment | 2.59 D |
| Thermochemistry | |
| Std molar entropy (S⦵298) | 354.2 J·mol⁻¹·K⁻¹ |
| Std enthalpy of formation (ΔfH⦵298) | -843.1 kJ/mol |
| Pharmacology | |
| ATC code | L01AB01 |
| Hazards | |
| Main hazards | Toxic if swallowed, fatal if inhaled, may cause genetic defects, may cause cancer. |
| GHS labelling | GHS02, GHS06, GHS08 |
| Pictograms | GHS06,GHS08 |
| Signal word | Danger |
| Hazard statements | H301 + H331: Toxic if swallowed or if inhaled. |
| Precautionary statements | P201, P202, P260, P264, P270, P280, P308+P313, P405, P501 |
| NFPA 704 (fire diamond) | 2-2-2 |
| Flash point | 89.3°C |
| Lethal dose or concentration | LD50 (oral, rat): 10 mg/kg |
| LD50 (median dose) | LD50: 10 mg/kg (oral, rat) |
| NIOSH | VZ1300000 |
| PEL (Permissible) | PEL (Permissible Exposure Limit) for Busulfan: "0.1 mg/m³ |
| REL (Recommended) | 60 mg/m³ |
| IDLH (Immediate danger) | IDLH: 60 mg/m³ |
| Related compounds | |
| Related compounds |
Treosulfan Ifosfamide Cyclophosphamide Melphalan Chlorambucil |
